Wednesday, December 21, 2005
Almost one year.
Monday, December 19, 2005
Hmm...
Sunday, December 18, 2005
Christmas Party
Where does one conscience go under anesthesia?
First of all not to nitpick but you probably mean consciousness, meaning sense of one's personal or collective identity, rather than conscience, meaning source of moral or ethical judgement. I only clarify this not to be a jerk, but to make sure we are on the same page.
I don't know if there's really a right answer to this question... First. Is this is the same quesion as "Where does one's consciousness go when I sleep?" Probably in my opinion. Anesthesia is induced sleep (more or less... i can give you a more techically specific definition but that will just be cumbersome in this metaphysical question)
Most would say one's consciousness is just supressed while you sleep or are under anesthesia... it's there but it's unable to express itself or take in new information.
More religious people would say it's there watching over you. A "soul" if you will.
Which is right? I don't know. Is there another alternative? I think the best thing would be to leave it comments and see what people have to say.
Monday, December 05, 2005
Level 1Trauma
Now I'm always kinda pissed off when I get called in... half the time I get called in for cardiac it's nothing critical (i know that sounds weird) Someone freaking out for no reason. I know it's my job to be available when they call me in, so I don't think i should be angry.... I still am. I figured if that bullet were anywhere important they'd be dead by now. I'm also mad for other people too. I think "Heaven forbid if anyone gets hurt driving in the snow coming into the hospital for this non-emergent 'emergency' "
I slip and slide my way in. I see the cardiac surgeon in the pump room. I say "hi, what's going on?" He says "I don't know... they told me she was dying and to come in, now we're waiting... i don't know what doing..." Great now the cardiac surgeon and I both don't know what's happening. Oh well easy enough to blame the Trauma service.
The patient finally shows up. Very stable. We put some invasive monitors and access into the patient. I don't see much blood in the pericardium (sac around the heart) on echo. There is some though... not much. Surgeon says it probably looked like pericardial fat because it was well-organzied clot. They take a closer look at the heart... this lady's lucky. The bullet went through the pericardium nicked the right side of the heart and kept going. A half-centimeter another direction and that nick would have gone through one of the coronary arteries and the patient would have bled to death or part of the heart would have completely stopped working. Lucky.
I feel bad now that I was angry driving in.
Wednesday, November 30, 2005
PACU
Not a typical day for me. I was the faculty covering the post-operative recovery unit. It's actually not a particularly tough job most of the time since there is a resident assigned to field most questions and problems. There's the occasional problem... nothing big today. Staffing ECTs. (electroconvusive therapy) Done three times a week in the PACU. Signing patients out (i.e. administrative whatever-you-want-to-call-it)
One thing that was unusual was that we had two physicians come through as patients. I guess doctors need surgery too. Didn't want to give special treatment, but did stop by and say hi to both the pediatric anesthesiologist and the cardiac surgeon (who spent the previous saturday on a stretcher in the pump room while his partner finished a surgery they had started together).
Tuesday, November 29, 2005
Bladder cancer
I'll be badder without a bladder!

Saturday, November 19, 2005
Tough Day
Anyway... the new heart is in the patient about 3 pm or so. It's not going well as we come off bypass, but we're doing reasonably. All of a sudden, the blood pressure drops and I see a bunch of air on the echocardiogram. Part of the hears stops functioning well... So I assume some air has gone down one of the coronary arteries. We crash back on bypass... Left heart starts functioning a bit better but now the right side doesn't look so well. We end up after struggling a bit assisting the right side of the heart with Abiomed right ventricular assist device. This are settling out, the all of a sudden the left side of the heart is starting to look bad.... Now a discussion ensues on if they need to put the patient on ECMO (extacorporeal membrane oxygenation). Ends up they endup supporting the left side of heart with a left sided Abiomed.
Now we are supporting both sides of the heart, and the patient is relatively stable We're pouring clotting factors and blood so the patient will stop bleeding. They'll try to wean the patient off assistance early next week. So this patient came into the hospital with a bad heart and a Left ventricular assist device... now has a different heart and assistance for both sides of the heart. Only time will tell. By the way it's 9pm we're finally done. a quick 16 hour case. I'm so exhausted.
Sunday, November 13, 2005
Interviews
Friday, November 11, 2005
Make a wish
The reason I remember this kid is that he was truely one in a million. The surgery he was having as an eight year old was a coronary artery bypass. He had a disease called hereditary familial hypercholesterolemia. The problem for this kid was that he had the worst kind. He had cholesterol levels 8 to 10 times what a normal person would have, thus he had premature disease of the arteries feeding his heart. Most patients who have this type of surgery are in their fifties and above.
What killed me was that on the news report they did say he had coronary artery disease, but they said that "Sometimes he doesn't feel well" and left it at that. I guess you can't say "Sometimes his heart doesn't get enough blood" on TV. Well at least he got a new puppy.
Tuesday, November 08, 2005
More Prisoners
Now I understand this guy is a violent criminal, but they bring this guy up to the OR... he's intubated and paralyzed... big wad of bloody bandages on his neck... but despite this fact he still has his arms shackled to his waist. Like he's getting anywhere while he's paralyzed. Then again with the sitting outside the OR while he's under general anesthesia. Oh well. I'm sure the guards are just doing what they're told.
Good news for us, he didn't hit anything too big that we couldn't control the bleeding. (plus they had time to fly him in from up north in the helicopter). Bad news for him... seems like he didn't feel like living anymore.
P.S. I was ending another case with a CRNA and she had only heard part of the story so she only knew we were operating on a self inflicted neck wound. So she said "Life can't be that bad can it?" I then mentioned that he was a prisoner apparently in prison for violent crimes. She then seemed embarrassed "I guess it can be that bad." I chuckled. (proves again -- I'm a bad man)
Tuesday, November 01, 2005
prisoners in the OR
A couple of years ago I had a patient undergoing cardiac surgery he was in his mid-seventies. Apparently he had been in prison for twenty or more years. He was a pretty feeble man... still those guards were there sitting outside the OR for the entire case. I really don't know what he did if he had been in prison for that long. He also seemed very nice.
Monday, October 17, 2005
Awful
On another note, the cardiac case I'm supervising finished early today. Which is good, but it's bad because that means our room is open for add-on cases which are always always always a mess. But our OR bed is broken so I'm hoping nothing comes. I'm a bad man.
Sunday, October 16, 2005
Music in the OR part deux
Anyway... it linked to a version of the article and asked why would anesthesiologists cooperate with publicity that that makes it look like they have nothing better to do in the OR other than play music. I never really thought about it that way. We usually are busy doing other stuff. still having a choice would be nice.
On a completely random note, had a pretty decent day on Friday. Working with two very good, very pleasant residents. One paged me because our "healthy" patient had just had a run of V-Tach... for those of you who are non-medical. It's heart rhythm that's potentially fatal if it persists and is untreated. Luckily in this instance it was short and self limiting, but we were sending off some lab tests to make sure it wasn't a fairly simple electrolyte problem. Anyway I threatened the resident with a bad eval if it happened again. I told her I would note on her eval that, "Resident was good to work with, very knowledgeable, but unfortunately arrythmogenic" (irregular heartbeat-causing) She laughed.... I think she was humoring me... then again she laughs at everything.
Tuesday, October 11, 2005
Music in the OR

Image provided by Freefoto.com
A friend of mine sent me this link...
Are anesthesiologists the DJs of the operating room?
At my hospital the surgeons have control over the music. No choosing by me. I don't think they'd like my music anyway. Hip hop and pop is probably to contemporary for the ORs.
There is a lot of music in the ORs... You can tell what kind of day you're going to be having depending on the music. Country in the Vascular rooms, a little bit of everything in the Neuro rooms... quiet only in Cardiac... music maybe when they're closing.
Sunday, September 25, 2005
House
Check out the House review at Polite Dissent
Tuesday, September 20, 2005
Enthusiasm
We were in the cardiac room... staffing is one on one in cardiac in our institution meaning we supervise only one cardiac case at a time. The second cardiac case of the day was supposed to be there already so they could get some invasive lines placed preoperatively. Usually the timing in such so that the most critical portion of the cardiac case is happening while I need to be surpervising those lines elsewhere. Anyway, came off of bypass in the OR, then finally then next patient was ready to get lined. After the lines were placed, I got back to the OR and they were about to transport the cardiac case to the ICU.
I told the resident to go to lunch (we give the breaks when we staff one on one) because I figured that i would get a chance for a couple more hours if he didn't go right away. He came back about 10 minutes early and met me in the ICU. Apparently he had bought me lunch and left it for me down in the anesthesia offices. Way beyond the call of duty... I suppose it's good for brownie points, but I don't believe he did it for that reason. I believe he did it just because he's a nice guy.
Glad there are still people out there like that.
Friday, September 09, 2005
Tuesday, September 06, 2005
Whoa
Wednesday, August 31, 2005
Bier Block
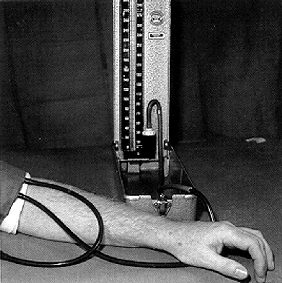
Image used without permission, property of original owner
We did a Bier Block yesterday. My new resident was very excited about it... I don't know if he's just an enthusiastic person or if the procedure was all that interesting. I guess we don't do that many of them, plus he's kind of new. Actually it's probably him... he IS very enthusiastic.
For those of you not familiar with the Bier Block it's named after Karl August Bier... some German guy who invented the technique in 1908. It's also called an intravenous regional anesthetic. It's useful only for surgeries on the extremities. Basically you put a pressure cuff on the arm, use a rubber bandage to squeeze out all the blood out of the arm. Then you inflate the cuff and inject local anesthetic into the arm (through an IV you've placed earlier in the hand) The arm stays numb as long as the cuff is holding the local in the arm. This works because in general nerves travel along with blood vessels in most of the body. So if you fill the vessels with local anesthetic, you also anesthetize the nerves.
Anyway now if I can just get that resident to stop calling me "Sir" we'll be in good shape.
Tuesday, August 30, 2005
Hurricane Katrina

Images from AFP/NOAA-HO used without permission
I'm watching the coverage of the damage caused by Hurricane Katrina. Makes me glad I live in the north... Makes a lot of my problems seem insignificant.
Interesting to hear that many more will die in the aftermath from lack of power and water and food etc.
Tragic. Mother Nature is a vengeful woman.
Friday, August 19, 2005
Avoiding the pain of death
This has been much different from my experience. I of course am in a different field. There is much more "volatility" in anesthesia. We deal with critical patients all the time. I, myself, have had particularly bad luck in this respect. I watched one of my patients bleed to death on my first day of anesthesia residency. It was very traumatic. I considered not coming back for a second day. Then I realized that was part of the job that I come there to do. I still remember that day vividly. I don't think i've had a case that bad since. I also had a patient die my first call as a attending staff. We did everything we could to keep that patient alive for three hours, but nothing helped. That was also very "character-building".
So how do we avoid death as physicians? The only way I can think is to avoid taking care of patients. I could quit tomorrow to drive a cab or work at Blockbuster. At what cost? I could throw away years of schooling and hard work, I could throw out the desire to practice good medicine. Unacceptable. I enjoy my work, but as a result I need to be able to deal with death. Hopefully not very often though.
My friend needs to learn this too... I think she'll come around. She's worked hard to get where she is... unfortunately she's pretty miserable these days. Hopefully as she gets further into her residency she will enjoy her work as much as I enjoy mine.
Sunday, August 14, 2005
Monster Garage
Image taken from Thoratec Corporation website without permission. Image property of Thoratec Corporation
I've been a full time cardiac anesthesia staff now for about a month. I thought I would be spending more time in the heart room, but it only ends up being about one day a week. Oh well. i don't mind the general ORs.
Wednesday was an interesting day in the OR. Two big cases by the newest cardiac surgical staff -- he just started in July, the same time as I did. They're giving him pretty big cases even though he's the most junior. Maybe it's a way of breaking him in or something. I don't know.
Our first case was an exchange of an abiomed LVAD for a heartmate LVAD. LVAD stands for left ventricular assist device. It's type of support to help the heart when it can't function well enough on its own. The difference between the two devices is that the first is a mini-fridge size device that sits next to the bed and has tubes connecting it to the heart... the second is an implantable device (think softball sized tuna can) connected to the heart to help pump. Patients with this devices can even go home. Mostly it's used as a bridge to transplantation. It wasn't a terribly long case, but it can be complicated. There's multiple vasoactive medications, nitric oxide, and a transesophageal echocardiogram to deal with. Also a tangle of IVs and lines. Went very well though.
The second patient had an even sicker heart. He had a Heartmate LVAD(see above) supporting his left heart and a abiomed RVAD (right ventricular assist device) supporting his right heart. He had recovered enough function in his right heart to have the RVAD removed. There's no cardiopulmonary bypass, but you have to deal with the possibility of a lot of bleeding. ALso the possibility exists that the right heart isn't ready to come off support yet and will fail after you cut off support. Again it went pretty well so I can't complain. But there's a lot to think about and take care of. I guess that's why I like being in the cardiac ORs
Monday, August 01, 2005
Dinner with my mentees
Thursday, July 28, 2005
horrible
(apologies for the extremely lingo filled post. had to vent.)
on the plus side went to have arab food with my buddy who finished his cardiac anesthesia fellowship. it was a good time, tasty food, good conversation, damn road construction detours though.
Thursday, July 21, 2005
new residents
Heard from a resident in the ICU
ECMO is easy, you just got to keep them from bleeding to death, and keep them from clotting to death.
(ECMO = Extracorporeal Membrane Oxygenation... more on ECMO another day... so complicated)
Thursday, July 14, 2005
Insanity
Thursday, July 07, 2005
Mentees
I am wondering why if there are dozens of faculty members why I got assigned two residents out of twenty-four to be mentees. Whatever... I don't really mind.
Saturday, July 02, 2005
First Day?
Sunday, June 19, 2005
Graduation
At the end of the month, I am no longer a cardiac anesthesiology fellow... I am a cardiac anesthesiology faculty.
A little bit of a strange feeling. Last year's graduation from residency was more significant. A bigger milestone, and I won an award I wasn't expecting. But it wasn't the end. I knew there was more.
Now there's no more. Just the "real world"
Scary.
happy dad's day

Thanks for all you've done.
What do you get the man that's made it possible for you to have all that you need?
My dad got DVDs. A small token. Thanks
Monday, June 13, 2005
Tamponade
I've been on cardiac call this weekend (as faculty). This means I sit at home waiting for my pager to go off, dreading any possible emergency cardiac cases that come in. I'm usually a wreck all weekend for two reasons. One, i know as soon as I plan to do something like meet friends for lunch or go to a movie, Murphy's law will kick in and I will get called in. Two, as a relatively new cardiac faculty, I'm probably not as confident in my skills as I should be and I have doubts about whether I can handle what comes it.
At 2:45 this morning. I get a page... "emergency bring-back bleed.... phone number blah blah blah" I call in and someone's coming straight down from the ICU. Now this isn't all that unusual. People have heart surgeries all week long, and sometimes they bleed more than they should afterwards. They ooze for a few hours, they are indecisive about coming to the OR... finally in the middle of the night they decide they've had enough and need to operate. They come down to the OR, the surgeons poke around a little and they use their electrocautery to buzz a few little blood vessels, say they can't find much, and then you go back upstairs. No big deal. The reason this is considered an emergency is that there is a possibility that there is a major bleed somewhere and it can compromise the way the heart functions. The heart can stop working because there can be blood clot all around it (rather than blood pumping through it)
So I assume it's one of those slow oozing bleeders, but you need to come in anyway and take care of the problem. I roll out of bed, do my best to fix my bed head and hop in the car. I'm at the hospital within 15 minutes, and changed in the locker room less than 10 minutes later. I walk into the OR expecting the nurses to be setting up and waiting for me to bring the patient down. Instead I see the general call residents and staff hovering around the patient. She's pale looking and her eyes look like they're half rolled back in her head. Now I'm thinking "aw, crap... this is for real" The cardiac surgery resident is throwing a few lines and we're scrambling to get this patient ready for surgery.
Now this is one of the special circumstances in anesthesia. You need to have the patient ready for surgery BEFORE they go to sleep. These compromised patients are using all their reserve to keep up their blood pressure, catecholamines rushing though their systems, peripheral vessels clamped down, all trying to compensate for this unstable state. When you put them asleep this relaxes their compensation and they can "crash" as soon as they're asleep. Also our medications to put you asleep tend to lower your blood pressure too. So to combat this, you have them prepped and drapped for surgery with the surgeon standing there ready to operate as soon as they are unconscious.
The cardiac surgeon pops his head it to see what's going on. His resident lets him know that this is the heart transplant patient from earlier in the week and that they need to get started NOW. They wash hand quickly while the nurses rush to prep the field. The drapes go up. And they let me know they're ready. I put the patient asleep and they get started immediately. My anesthesia resident puts in the breathing tube under the drapes and the surgeons open up the chest. Immediately you can see blood welling up out of the chest and a squirting bleeder. Immediately the blood pressure drops. We've lost about 2 liters of blood in about 10 seconds. We get the rapid infuser going and pump in some blood quickly and I give the patient some epinephrine(one of our stronger drugs) to get the blood pressure back up. Luckily they get the bleeder under control and about 2 hours later we get back up to the ICU.
We were pretty lucky today. I can help but think that if it had taken me 10 more minutes to drive in, or that if the team in the hospital hadn't been so proactive in getting the patient to the operating room that this lady might be dead. I'm relieved.
It's 530 am. I'm tired, i'm thinking of going home. I over hear the cardiac surgery resident, "blah blah blah accepted a lung transplant blah blah blah..." I know I'll be back later today.
Monday, June 06, 2005
Running
The thoracic room has two moderately sized cases... requiring epidurals and alines.
The ENT room has 6 short cases, at least 2 requiring awake fiberoptic intubation.
The kicker? The two rooms are about as far apart as you can get in the ORs. My room assignments got switched today because they opened up a 3rd cardiac room. I'll be running my ass off tomorrow. If i'm smart i'll pack a lunch. I probably won't though.
Sunday, May 22, 2005
Happy Birthday Morphine!
Kelly did not forget and collected some anecdotes in honor of morphine's birthday.
I'll send a card later.
Wednesday, May 18, 2005
Tangled Bank
Wednesday, May 11, 2005
Blogging when people you know read your blog
25) Given that there are plenty of people who've been fired or disciplined at work either for blogging on the job or for something they said on their blog, the fewer people at your job who know about your blog, the better.
I know at least 2 people at work know of my blog... should it affect how I blog... probably not. Does it... probably. I not only have to worry about getting fired. I have to worry about being sued and patient confidentiality. I don't blog at work.
Coincidentally... a friend of mine who has an incredibly insightful blog (and she didn't want to tell me about it -- I haven't linked to her at her request) said yesterday.
Even now, I am concious of what I write because of those who know about it or have ever visited it that may know me.
I think it affects what I write as well. One of the comments from the first article said it best.
Blog because you want to, ...It's the passion that readers will respond to.
Blog on.
Sunday, May 08, 2005
Thursday, May 05, 2005
Vomiting Ferrets?

Fidgett the ferret (maybe it's Waffles the ferret... i don't know them so I can't tell) from ToyKeeper.net. Images used without permision
Today while hanging out with some of my smart friends, I learned randomly that ferrets apparently are used in lot of research for nausea and vomitting. I thought this to be rather strange. I also began to have images of a cage some where with liitle piles of ferret vomit in the corners.
I began also to wonder why this is. So I went to our friend the internet...
Most animal research on nausea is performed on ferrets, apparently one step up the evolutionary tree from rodents, which do not vomit.
-- From Palliative Care Perspectives, James L. Hallenbeck, M.D.
Saturday, April 30, 2005
Juggling
Logo of the 6th Swiss Juggling Convention, in Zürich 1992, used without permission
So I feel like I'm not getting enough done.
I'm trying to buy a house, do a good job at work, study for boards, read to prepare for talks, plan a vacation with some college friends... all while trying to get enough sleep and also not go insane, which means decompression time.
Mortgage insurance, home inspection, radon, homeowners insurance, down payment, closing costs, argh!
They say life events are very stressful. Several are going on now. I don't even have kids or a wife or girlfriend to distract me. I've been neglect the cat. I don't know how some people do it. They are amazing.
Damn, I need a haircut too.
Sunday, April 24, 2005
Board Review

Image used without permission from USGS via Wikipedia.org
Just got back from an intensive 3 1/2 day Board Review Course in Chicago. It kicked my butt. I hope I'm ready in 10 weeks. I've gotten great traning in anesthesia, but I still don't feel ready to take the boards (again). The course was worth the extensive fee though. We'll see if it was really worth it when I get my scores.
Sunday, April 17, 2005
Trick Daddy
Lately on the radio they've been playing (Gimme Some) Sugar(remix) by Trick Daddy, featuring Ludacris, Lil' Kim, and Cee-Lo. It's a great song. They have some amazing rhymes.
One verse by Lil' Kim goes "I give ya high blood pressure like a diabetic". I know they're trying to relate the diabetes theme in as the title is Gimme Some Sugar, but I don't know that diabetes cause hypertension. They are associated however it seems. I guess she's saying she's so hot she raises your blood pressure.
Oh well, I can't hold it against them. I still like the genre. I still like the song.
Thursday, April 14, 2005
Litigation
There are several things that would have to occur to make this a successful suit.
First of all, it requires a bad relationship with the patient. In this case, it was fully explained to the patient, and the procedure to correct the problem was immediately arranged. The patient seemed very understanding. For the second reason we need to go to my lawyer buddies.
A tort is a wrongful act other than a breach of contract that injures another and for which the law imposes civil liability. There are four elements of a tort as I understand it
- Duty
- Breach of Duty
- Damages/Harm
- Causation
If all four are not present a tort should not be successful. In this case, there was a duty, and that duty was definitely breached. Most of the time, the act in question does not involve arguing breach of duty, it is assumed to have happened. There also needs to be damages or harm associated with the breach of duty, and the damages must be caused by the breach of duty. If there is no damages, there is no tort. If there are damages, but no causation, there is no tort. In this case, there were no damages to the patient other than having to go through the corrective procedure. So there should no sucesful tort possible.
PS. Hmmm...
looking through my visitor statistics, apparently I'm the 27th choice for a google search of the movie SuperSize Me. Interesting.
Tuesday, April 12, 2005
Monday, April 11, 2005
Difficult Airway
I'm sort of sleepy there looking at my laptop screen in the anesthesia library... and I hear "Anesthesia Staff Stat to ER!" This is not normal. This is usually our safety system in the OR, if something crazy is happening in the OR and you need emergency help or an extra hand, anyone can call overhead to get someone into the room. Residents, CRNAs, or even faculty anesthesiologists can call out and get help. i.e. "Anesthesia staff stat to OR 12." So to hear this page at all means something isn't going well. This is the first time I've heard this call to somewhere other than the OR. Usually that is reserved for the Anesthesia group pager or the code Blue pager. So I figure I'd better get off my butt and see if they need a hand. I walk quickly down the hall (I never run, because 1.If I fall on my face they'll be two patients instead of one 2.I'm out of shape ) A couple of other staff are headed the same way. One of them is relatively new and she doesn't even know where the ER is so she joins us. We cruise down the stairs, swipe our IDs through the security door and head toward the trauma bays. Quite a few others are there already in addition to the ER people, some various nurses and other doctors.
I look at the patient and you know they're in trouble. In medical circles it's sometimes referred to as FLK... funny looking kid... A small really tiny kid with small receding jaw with a massive overbite. Almost Pierre-Robin like in look (GIS for Pierre-Robin) I know immediately that he's going to be difficult to intubate. Now as misunderstood as I usually claim anesthesiology is, most would agree that in addition to the ENT surgeons, we are airway specialists. I see them take a look with a laryngoscope and they see nothing. They look with a fiberoptic scope and they see nothing... by now they've called ENT and peds ENT for a possible emergent tracheostomy. Peds anesthesia has been called to bring their code box and airway equipment. Lucky they are barely able to mask ventilate the patient. I also notice the scar on the patient's neck indicating a previous tracheostomy. They're still having no luck with using a fiberoptic scope for intubation. Incidentally someone mentions that this "kid" is 28 years old.... something like 60 pounds and change.
He's starting to breathe now. He had stopped breathing earlier for some still unknown reason. Seizures and sleep apnea are mentioned. Since he's breathing now and still maintaining his oxygen saturation we decide to get up to the OR where more instruments (and a more controlled setting) are available.
So we run up and this patient recieves and awake tracheostomy, which is the ultimate in secure airways. Ends up that this "kid" as an unknown syndrome and some history of autism (though lives on his own) and has been trached in the past for losing his airway during a seizure eight months ago.
This is an anesthesiologist's nightmare. We have all sorts of tricks and techniques to control the airway. But sometimes we fail. The trick is knowing when to call for help as a good senior anesthesiology resident did, and when you've tried things and they aren't working to call for a definitive surgical airway when necessary. It's hard to ask for help. In this case I think we saved this guy's life. Now someone just needs to figure out why he's having seizures (already on two anti-seizure medications)
Saturday, April 09, 2005
Garage?
Yesterday, a patient remarked as we rolled him into OR 6, "This is the operating room?? It looks like a garage!
Thursday, April 07, 2005
Dedication
Now I don't know if this is all true. I'm hearing it second hand. But i heard it from two people.
(BTW, he's a great surgeon)
Tuesday, April 05, 2005
Rounds
It's my first submission and post there...
If you're not familiar with term Grand Rounds... it's basically a conference where people talk about a particular subject or recent events in the department. Often there's a guest speaker or something. Evidently it's taken from John Hopkins hospital back in the day. The patient's rooms were in the rotunda and to see them you went "a round" Everything medical has to have "rounds" after it it seems
Seeing patients with your team before the attending arrives is "work rounds"
Seeing patients by yourself before work rounds is "pre-rounding"
Seeing patients with your attending is just "rounds"
Seeing patients with special attending for education purposes is "teaching rounds"
"Grand Rounds" is usually the department's weekly conference.
Eating is "p.o. (per ora) rounds"
Staffing friends
Also it it means staffing friends. I've become friends with a lot of the residents because we were in the same program before I was an attending, and we've remained friends. I try to be laid back about the whole process. This morning we bring the patient back into the room after the resident puts in an arterial line and thoracic epidural in the pre-op area. I look at the top of his cart. Now there's supposed to be a bunch of medications available for me to help put the patient asleep. And in addition there's supposed to be some emergency drugs there 'just in case' something happens. I look and there's a couple of syringes of paralytic sitting there. Nothing there to put the patient asleep, nothing to use in case of emergency. He turns and says he forgot the induction agent so we send our medical student running to the pharmacy while we put the patient on monitors. I didn't want to make a big deal of everything so I draw up some emergency drugs while he's fiddling with things. The student comes back and we put the patient asleep. We're getting things worked out and just comment to him that even though we're friends we need to be a little more prepared to do these cases. He gives me a funny look and chuckles. He points to his pocket and the emergency drugs are there ready to go. He says he was wondering why I drew up the other stuff. Ha ha.. now don't I look silly. SO STRESSFUL... people need to tell me things
Friday, April 01, 2005
Plane trouble
Tuesday, March 29, 2005
Eww!
Defecography is a test used to evaluate the disorders of the lower bowel that are not evident by direct visualization. Radiologic liquid is instilled into the rectum. Then the patient is instructed to empty the rectum while a fluoroscopic exam of the pelvis is carried out. This radiologic test allows the doctor to evaluate the pelvic floor muscles and rectum during defecation. This type of test, although awkward, provides valuable information that will aide your doctor in diagnosing your problem.
The following is a list of conditions for which Defecography can be used to gather more information and/or confirm a diagnosis.
-Rectal prolapse, irritable bowel syndrome, obstructed defecation
-Solitary rectal ulcer, proctalgia, fugax,a rectocele/enterocele
-Fecal incontinence, internal prolapse, constipation
-Rectal/anal intussusception anismus (inappropriate spasm of the anal sphincter)
(UMHS website)
Apparently the "liquid" they use for this test is the consistency of mashed potatoes.
Thank god I'm an anesthesiologist. I'm glad on the other end of the patient.
Sunday, March 27, 2005
Death
Supersize Me
(Really I'm just kidding. I haven't drank sugar soda in years.)
Wednesday, March 23, 2005
Extra room
Today was a bit different. The case that was scheduled in our room was cancelled so that a case that had been cancelled because of emergencies, scheduling, etc had been cancelled two days in a row could go. Unfortunately the original surgeon wasn't available so his colleague agreed to do the case for him. The patient wanted her surgeon to do the case, so she didn't want the case done today. So instead of one or two cases as usual, we had none. This you would think is a good thing. It's not. That means ANY case can be put in your room.
The day starts off with a page while I'm driving in that a cardiac case from yesterday needs to come down emergently for bleeding (well he's been bleeding all night) so I take over from the night staff. Usually in cardiac you are staffing one case/one resident at a time. Apparently there's some sort of flu going around (which I think I have, by the way) because two staff anesthesiologists call in sick (which never happens). We end up giving a bunch of clotting factors during the case, plasma, platelets, recombinant factor seven even (something like $5000 a dose) before the guy quits bleeding. As we're finishing up. I get a page. "Would you mind covering another room because we're short staffed?" I say sure no problem figuring they'd give me an easy room because 1) I'm a fairly new faculty and 2) I'm already covering a cardiac case (not a pump case but still) "So we have a ruptured aortic aneurysm coming in and by the way it's a relative of one of our nurse anesthetists" No pressure right? Yikes. If you don't know, a ruptured abdominal aortic aneurysm (AAA) is an anesthesiologist's (and surgeon's) nightmare. Only fifty percent of these patients even reach of the hospital. Another fifty percent of these never leave the OR, a fraction of those leave the hospital (alive that is) Luckily it ends up being a contained rupture of a previous endovascular AAA repair so it's much more stable than you'd think (which is good)
By this time. There are add-on's in my cardiac room. Not cardiac cases, but ENT cases instead followed by a neurosurgery case. bleah. PLUS i'm doing the to-follow vascular case in the other room. That's the breaks. Not bad for a day's work. I did get to leave fairly early for a call day despite the liver transplant added onto the schedule.
Sunday, March 20, 2005
Television
Cool eh? I'm famous!
Well not really. The Discovery Channel was at my hospital a few months ago filming stories about residents. I help in part of a heart transplant, so you can see the side of my head over the surgical drapes. Not that I want to be on TV, but they seem to gloss over the anesthesia portion of these cases a lot. Oh well. Surgery makes better television.
Wednesday, March 09, 2005
Trust
why?
Monday, March 07, 2005
British rotators
Sunday, February 27, 2005
Discovery Health
Saturday, February 19, 2005
Patient Management
I've seen situations where a patient has had surgery, received some fluid during the procedure, discharged home, and readmitted upto a week later, with a diagnosis of too much fluid during anesthesia when there are clearly other issues in play. A week later! I've seen surgeons blame anesthesia for kidney failure in a patient who had a liver transplant, when that is clearly a known complication during such an extensive operation. Seems to me that in particular surgeons are micro managers... at least in general... at least at the University level. I've had surgeons ask me to give blood products to patients at the same time not to raise the central venous pressure (which is a measure of volume status and raised directly by giving fluids or blood)
I'm not saying anesthesiologists are perfect. I'm saying that we've been to medical school too, and we've gone through specialized training. Give us a break.
Saturday, February 12, 2005
Heart trouble 2
Thursday, February 03, 2005
Thirsty
Later I'm giving the resident in the room a break while we're on bypass and I look at the intraoperative lab work. The hematocrit (aka "crit"), or percentage blood count, is 41 on the slip -- it's circled and the tech or perfusionist or someone had written "Outstanding!" next to it. This struck me as kind of funny. Someone was impressed enough with the lab value to comment about it.
A "normal" hematocrit is generally listed at 42-54 percent, but in my experience cardiac surgery patients tend to be a bit anemic and run in the 30-40 range. Now after you go onto bypass the hematocrit tends to drop a bit because the bypass pump is primed with fluid so the blood volume gets diluted and a hematocrit above 27 tends to be acceptable for most patients. Some patients start low and drop further on bypass and receive blood as a result. So 41 is really doing pretty good. I look back to the first set of labs before the patient is asleep and the crit is 48. Again still within the normal range, but quite a bit higher than we usually see for our cardiac patients. Explanations for this are many, and include disorders such as polycythemia vera where the blood is abnormally thick. In this clinically setting the most likely diagnosis is dehydration. In this instance, it was caused by us, in our instructions for the patient not to eat or drink.
So when this patient said he was thirsty... he really meant it.
Saturday, January 22, 2005
Heart trouble
Anyway he had an uneventful night in the hospital. And we picked him up at the hospital after being dumped on by 8-10 inches of snow. It sucks. I shoveled the driveway at home and after an hour I had to shovel another 2 inches off... what gives.
Thursday, January 20, 2005
Mortality
Yesterday my dad called me and told me had a positive stress test. That means that there is a high likelyhood that he has some blockage in some of the arteries of his heart. Tomorrow he's going in for a heart catheterization. They will place catheters in his groin, fish them up to the heart and then shoot dye into the arteries of the heart. If there is are blockages they may stent them open, or maybe he will need heart surgery, or maybe none of the above if the blockages are minor. All of these procedures carry their own risks. Likely tomorrow everything will be fine... but I've seen with my eyes bad things happen. Maybe I know too much. I rarely see the results at work of "normal" tests.
This brings somethings into perspective. Here I am. 29 years old. A physician. single. overweight. i don't exercise, i eat poorly. I think I need to make some changes. I've always known better. I just never had a reason to change.
Tuesday, January 18, 2005
kitty litter
Wednesday, January 12, 2005
Yay
I'll tell you about my other first days later.
Tuesday, January 11, 2005
First Days
Monday, January 10, 2005
Awareness under anesthesia
Most awareness situations occur due to drug error, which is easy enough because of all the different medications that we use. I've made drug errors, anyone who says they haven't is a liar. luckily nothing serious or life threatening has happened because of this, and I try to be careful.
As for awareness, most times it happens in trauma situations and cardiac anesthesia. During traumas, people don't always get a complete anesthetic for the reason that people are worried about keeping them alive. I say that I'd rather have some awareness and be alive then the other way around. As for cardiac anesthesia, I should be worried about thi more since that's my speciality. I think this is a result of the historical perspective of cardiac anesthesia. We tend to now use a much different combination of drugs then we did just five, ten years ago so I think this is less of a problem.
Anyone out there concerned about awareness during anesthesia... it's a valid concern. Awareness is a rare occurrence but it does happen. Talk to your anesthesiologist before your surgery and let them know your concerns. If you have some awareness after your surgery, let your anesthesiologist know! If you don't remember who he or she was, make the department aware of your problem and they should be able to put you in touch with your anesthesiologist. Sweet dreams?!
Sunday, January 09, 2005
Doctor aids juror, mistrial declared
NORWALK, Ohio (AP) — A judge declared a mistrial in a medical negligence case against a physician after the doctor came to the aid of a juror who passed out during opening statements.
The defendant, Dr. Joseph Carver, told the 74-year-old juror Wednesday that it appeared he had a heart flutter that momentarily prevented oxygen from getting to his brain and caused the blackout. The juror was taken to a hospital for tests.
No new trial date has been set.
Carver, an obstetrician and gynecologist, is being sued for $3 million by a couple who say their newborn daughter was dropped on the floor of a delivery room in 2000 while under Carver’s care.
They say the baby’s fall caused speech problems, seizures and other permanent neurological injuries.
The doctor can't be that bad of a doctor....
Thursday, January 06, 2005
I hate my job
What is my job really. I'm a cardiac anesthesiology fellow. Which means that I've finished training to be an anesthesiologist and that I'm doing speciality training to do predominatly anesthesia for heart surgery. I'm about half way done with my fellowship. This means I'm in the gray zone between being in charge of the case and just following directions.
Anyway, today we were doing a descending thoracic aortic aneurysm repair under hypothermic circulatory arrest. This probabaly requires some explaination. A portion of the biggest blood vessel in the body, the aorta, has enlarged to a size that risks rupture at any time. The surgeon was going to repair the portion of the aorta that comes down through the chest with artificially material. This requires putting the patient on a cardiopulmonary bypass machine (the "heart-lung" machine). The bypass machine does the work of the heart and lung while it is on. For this surgery, once on bypass, the body is cooled to 18 degrees centigrade. The head is than packed in ice to protect the brain and the bypass machine is shut off. This is the circulatory arrest portion. The surgeon then cuts out the diseased portion and repairs it quickly then returns to bypass. While the bypass machine is off, no blood is flowing through the body. The longer the bypass machine is off, the higher the risk of complications to the patient, including death or stroke.
Anesthesia for this surgery is quite complex as well as you can imagine. These patients require complex monitors to watch their status during the operation. These include a big IV, and arterial line to monitor blood pressure, an introducer in a vein in the neck to give lots of blood or fluids through, a pulmonary artery catheter to monitor their heart function during the operation, as well as a double lumen endotracheal tube to isolate each lung so that one lung can be deflated during the surgery. In addition to protect the spine during the procedure, we routinely put in a lumbar drain to take spinal fluid out from around the spinal cord. All in all... before the surgery starts, as anesthesiologists, sometimes we need 2 hours or more to put all the monitors in before the surgery even starts. That is, if all goes well. Sometimes it takes longer. Today it took longer. First of all, the patient had had a difficult intubation in the past. This meant we needed to use a fiberoptic scope to place a breathing tube in the patient. The other monitors went okay until we placed the spinal drain. Suffice it to say instead of a 20 minute procedure, we took almost three hours to place the damn thing. This ultimately included calling another anesthesiologist in, moving the patient to another bed, placing him prone and using xray flouroscopy to place the catheter.... once it was in, we had to move him back to the other bed and place him on his right side, so the operation could take place. Instead of starting the actual surgery at 10ish.(Thursday is a late start day), we started at almost 2pm. About 6 hours of preping this patient before the surgery even started. I wanted to scream.
It amazes me to think that we can do this surgery at all. I'm sure these people must have just died at home somewhere, or in the mall, or at the post office, not ever knowing there was a problem. It amazes me that we can do most of the procedures that it is possible for an anesthesiologist to do before 10 in the morning.
I love my job.
Wednesday, January 05, 2005
Hello
I'm not sure anyone understands what anesthesiologists do. Not even the surgeons with which we work every day. Even the title of this blog isn't quite right. Anesthesia isn't just about putting people to sleep. Sometimes it is... not always. Anyway. I have a lot of interesting stories from work. It shouldn't be overly technical or academic, at least not at first. Hopeful this will be an insightful and enjoyable journey. If not, I at least get a chance to vent. Feel free to send or make comments. I'll do my best to address them if anyone actually reads this.